Endometrial Cancer
The endometrium is the lining of the uterus, a hollow, muscular organ in a woman’s pelvis. The uterus is where a fetus grows. In most nonpregnant women, the uterus is about 3 inches long. The lower, narrow end of the uterus is the cervix, which leads to the vagina.
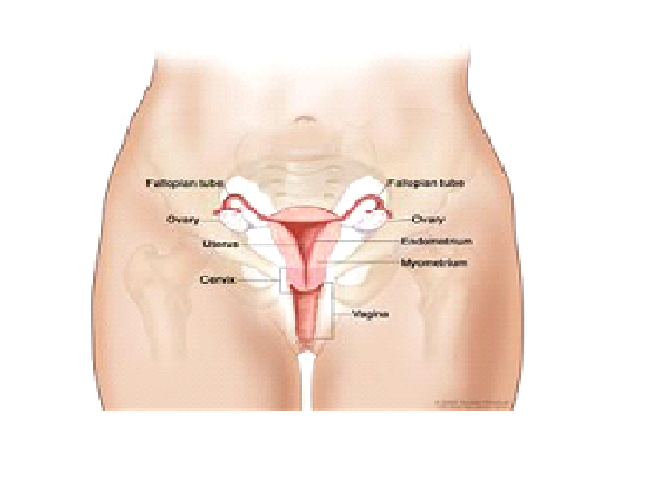
Anatomy of the female reproductive system. The organs in the female reproductive system include the uterus, ovaries, fallopian tubes, cervix, and vagina. The uterus has a muscular outer layer called the myometrium and an inner lining called the endometrium.
Cancer of the endometrium is different from cancer of the muscle of the uterus, which is called sarcoma of the uterus. Refer to the PDQ summary on Uterine Sarcoma Treatment for more information.
Taking tamoxifen for breast cancer or taking estrogen alone (without progesterone) can affect the risk of developing endometrial cancer.
Endometrial cancer may develop in breast cancer patients who have been treated with tamoxifen. A patient taking this drug should have a pelvic exam every year and report any vaginal bleeding (other than menstrual bleeding) as soon as possible. Women taking estrogen (a hormone that can affect the growth of some cancers) alone have an increased risk of developing endometrial cancer. Taking estrogen in combination with progesterone (another hormone) does not increase a woman’s risk of this cancer.
Possible signs of endometrial cancer include unusual vaginal discharge or pain in the pelvis.
- Bleeding or discharge not related to menstruation (periods).
- Difficult or painful urination.
- Pain during sexual intercourse.
- Pain in the pelvic area.
Tests that examine the endometrium are used to detect (find) and diagnose endometrial cancer.
- Endometrial biopsy: The removal of tissue from the endometrium (inner lining of the uterus) by inserting a thin, flexible tube through the cervix and into the uterus. The tube is used to gently scrape a small amount of tissue from the endometrium and then remove the tissue samples. A pathologist views the tissue under a microscope to look for cancer cells.
- Dilatation and curettage: Surgery to remove samples of tissue or the inner lining of the uterus. The cervix is dilated and a curette (spoon-shaped instrument) is inserted into the uterus to remove tissue. Tissue samples may be taken and checked under a microscope for signs of disease. This procedure is also called a D&C.
Certain factors affect prognosis (chance of recovery) and treatment options.
- The stage of the cancer (whether it is in the endometrium only, involves the whole uterus, or has spread to other places in the body).
- How the cancer cells look under a microscope.
- Whether the cancer cells are affected by progesterone.
Endometrial cancer is highly curable.
Stages of Endometrial Cancer
After endometrial cancer has been diagnosed, tests are done to find out if cancer cells have spread within the uterus or to other parts of the body.
The process used to find out whether the cancer has spread within the uterus or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. Certain tests and procedures are used in the staging process. A hysterectomy (an operation in which the uterus is removed) will usually be done to help find out how far the cancer has spread.
There are three ways that cancer spreads in the body.
- The three ways that cancer spreads in the body are:
- Through tissue. Cancer invades the surrounding normal tissue.Through the lymph system. Cancer invades the lymph system and travels through the lymph vessels to other places in the body.
- Through the blood. Cancer invades the veins and capillaries and travels through the blood to other places in the body.
When cancer cells break away from the primary (original) tumor and travel through the lymph or blood to other places in the body, another (secondary) tumor may form. This process is called metastasis. The secondary (metastatic) tumor is the same type of cancer as the primary tumor. For example, if breast cancer spreads to the bones, the cancer cells in the bones are actually breast cancer cells. The disease is metastatic breast cancer, not bone cancer.
The following stages are used for endometrial cancer:
Stage I
In stage I, cancer is found in the uterus only. Stage I is divided into stages IA, IB, and IC, based on how far the cancer has spread.
- Stage IA: Cancer is in the endometrium only.
- Stage IB: Cancer has spread into the inner half of the myometrium (muscle layer of the uterus).
- Stage IC: Cancer has spread into the outer half of the myometrium.
Stage II
In stage II, cancer has spread from the uterus to the cervix, but has not spread outside the uterus. Stage II is divided into stages IIA and IIB, based on how far the cancer has spread into the cervix.
- Stage IIA: Cancer has spread to the glands where the cervix and uterus meet.
- Stage IIB: Cancer has spread into the connective tissue of the cervix.
Stage III
In stage III, cancer has spread beyond the uterus and cervix, but has not spread beyond the pelvis. Stage III is divided into stages IIIA, IIIB, and IIIC, based on how far the cancer has spread within the pelvis.
Stage IIIA: Cancer has spread to one or more of the following:
- the outermost layer of the uterus; or
- tissue just beyond the uterus; or
- the peritoneum.
0) Stage IIIB: Cancer has spread beyond the uterus and cervix, into the vagina.
1) Stage IIIC: Cancer has spread to lymph nodes near the uterus.
Stage IV
In stage IV, cancer has spread beyond the pelvis. Stage IV is divided into stages IVA and IVB, based on how far the cancer has spread.
- Stage IVA: Cancer has spread to the bladder and/or bowel wall.
- Stage IVB: Cancer has spread to other parts of the body beyond the pelvis, including lymph nodes in the abdomen and/or groin.
- Recurrent Endometrial Cancer
- Recurrent endometrial cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the pelvis, in lymph nodes in the abdomen, or in other parts of the body.
Treatment Option Overview
Different types of treatment are available for patients with endometrial cancer. Some treatments are standard (the currently used treatment).
Three types of standard treatment are used:
Surgery
Surgery (removing the cancer in an operation) is the most common treatment for endometrial cancer. The following surgical procedures may be used:
- Total hysterectomy: Surgery to remove the uterus, including the cervix. If the uterus and cervix are taken out through the vagina, the operation is called a vaginal hysterectomy. If the uterus and cervix are taken out through a large incision (cut) in the abdomen, the operation is called a total abdominal hysterectomy. If the uterus and cervix are taken out through a small incision (cut) in the abdomen using a laparoscope, the operation is called a total laparoscopic hysterectomy.
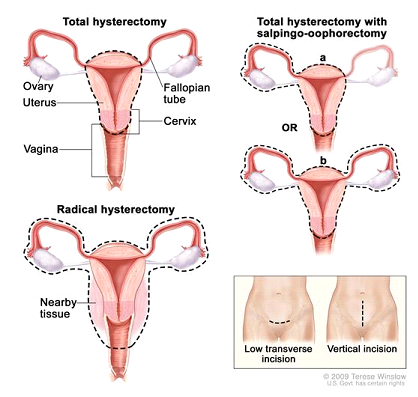
Hysterectomy. The uterus is surgically removed with or without other organs or tissues. In a total hysterectomy, the uterus and cervix are removed. In a total hysterectomy with salpingo-oophorectomy, (a) the uterus plus one (unilateral) ovary and fallopian tube are removed; or (b) the uterus plus both (bilateral) ovaries and fallopian tubes are removed. In a radical hysterectomy, the uterus, cervix, both ovaries, both fallopian tubes, and nearby tissue are removed. These procedures are done using a low transverse incision or a vertical incision.
- Bilateral salpingo-oophorectomy: Surgery to remove both ovaries and both fallopian tubes.
- Radical hysterectomy: Surgery to remove the uterus, cervix, and part of the vagina. The ovaries, fallopian tubes, or nearby lymph nodes may also be removed.
Even if the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given radiation therapy or hormone treatment after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. The way the radiation therapy is given depends on the type and stage of the cancer being treated.
Hormone therapy
Hormone therapy is a cancer treatment that removes hormones or blocks their action and stops cancer cells from growing. Hormones are substances made by glands in the body and circulated in the bloodstream. Some hormones can cause certain cancers to grow. If tests show that the cancer cells have places where hormones can attach (receptors), drugs, surgery, or radiation therapy are used to reduce the production of hormones or block them from working.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the spinal column, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Treatment Options by Stage
Stage I Endometrial Cancer
Treatment of stage I endometrial cancer may include the following:
- Surgery (total abdominal hysterectomy and bilateral salpingo-oophorectomy). Lymph nodes in the pelvis and abdomen may also be removed for examination under a microscope to check for cancer cells.
- Surgery (total abdominal hysterectomy and bilateral salpingo-oophorectomy, with or without removal of lymph nodes in the pelvis and abdomen) followed by internal radiation therapy or external radiation therapy to the pelvis. After surgery, a plastic cylinder containing a source of radiation may be placed in the vagina to kill any remaining cancer cells.
Radiation therapy alone for patients who cannot have surgery.
Stage II Endometrial Cancer
Treatment of stage IIA endometrial cancer is usually a combination of therapies, including internal and external radiation therapy and surgery.
Stage IIA
Treatment of stage IIA endometrial cancer may include the following:
- Surgery (total abdominal hysterectomy and bilateral salpingo-oophorectomy). Lymph nodes in the pelvis and abdomen may also be removed for examination under a microscope to check for cancer cells.
- Surgery (total abdominal hysterectomy and bilateral salpingo-oophorectomy, with or without removal of lymph nodes in the pelvis and abdomen) followed by internal radiation therapy or external radiation therapy to the pelvis. After surgery, a plastic cylinder containing a source of radiation may be placed in the vagina to kill any remaining cancer cells.
- Radiation therapy alone for patients who cannot have surgery.
Stage IIB
Treatment of stage IIB endometrial cancer may include the following:
- Surgery (total abdominal hysterectomy, bilateral salpingo-oophorectomy, and removal of lymph nodes in the pelvis and abdomen for examination under a microscope to check for cancer cells) followed by radiation therapy.
- Internal radiation therapy and external radiation therapy, followed by surgery (hysterectomy and bilateral salpingo-oophorectomy, and removal of lymph nodes in the pelvis and abdomen for examination under a microscope to check for cancer cells).
- Surgery (radical hysterectomy with or without removal of lymph nodes in the pelvis for examination under a microscope to check for cancer cells).
Stage III Endometrial Cancer
Treatment of stage III endometrial cancer may include the following:
- Surgery (radical hysterectomy and removal of lymph nodes in the pelvis for examination under a microscope to check for cancer cells) followed by internal radiation therapy and external radiation therapy.
- Radiation therapy alone for patients who cannot have surgery.
- Hormone therapy for patients who cannot have surgery or radiation therapy.
Stage IV Endometrial Cancer
Treatment of stage IV endometrial cancer may include the following:
- Internal radiation therapy and external radiation therapy.
- Hormone therapy.
Treatment Options for Recurrent Endometrial Cancer
Treatment of recurrent endometrial cancer may include the following:
- Radiation therapy as palliative therapy to relieve symptoms and improve the patient’s quality of life.
- Hormone therapy.